Original Article
Year: 2021 |Volume: 2 | Issue: 06 |Pages: 12-23
COMPARATIVE STUDY TO EVALUATE THE EFFICACY OF KOLAKULATTHADI CHURNA PINDA SWEDA AND ERANDMOOLA CHURNA PINDA SWEDA ON AVABAHUKA WITH SPECIAL REFERENCE TO FROZEN SHOULDER
About Author
Correspondence Address:
Dr.Sumit Ingole SDM’s Trust Ayurvedic Medical College, Terdal (Karnataka) Mobile no: 98902 39264
Date of Acceptance: 2021-06-02
Date of Publication:2021-07-30
Article-ID:IJIM_78_07_21 http://ijim.co.in
Source of Support: Nil
Conflict of Interest: None Declared
How To Cite This Article: Ingole Sumit. Comparative Study to Evaluate the Efficacy of Kolakulatthadi Churna Pinda Sweda and Erandmoola Churna Pinda Sweda on Avabahuka with special reference to Frozen Shoulder. Int. J Ind. Med. 2021;2(6):12-23
Abstract
Introduction: Avabahuka is one such disease that hampers the day-to-day activity of an individual. Avabahuka is a disease that usually affects the shoulder joint (Amsa Sandhi) and is produced by the Vata dosha. Objectives: To study the efficacy to evaluate the Efficacy of Kolakulatthadi Churna and Erandmoola Churna Pinda Pinda Sweda on Avabahuka. To compare the efficacy Kolakulatthadi Churna Pinda Sweda and Erandmoola Churna Pinda Sweda on Avabahuka. Methodology: In this study, 40 patients of Avabahuka were selected randomly and Group-A of 20 Patients received Kolakulatthadi Churna Pinda Sweda while Group-B received Erandmoola Churna Pinda Sweda for 30 minute for 14 days. Results & discussion: In Group-A, percentage of relief noted in Ansasandhi Shula was 77.3%, while relief observed in Ansa Sthabdata, Bahu Shosha, Sanchari vedana, In Group-B, percentage of relief observed in Ansasandhi Shula was 59.5%, while relief observed in Ansa Sthabdata, Bahu Shosha. Average relief observed in Group-A in subjective criteria was 74.4% while in objective criteria it was 57%. Average relief in both criteria was 67%. Average relief observed in Group -B in subjective criteria was 72.3% while in objective criteria it was 75.7%. Average relief in both criteria was 73.7%. It was observed that, in Group-A and Group B, regarding symptom Ansasandhi Shula, Ansa Sthabdata, Bahu Shosha and Sancharivedana was statistically highly significant within group. In symptoms Ansasandhi Shula, Ansa Sthabdata, Bahu shosha, Sancharivedana shows difference was considerably not significant.
Conclusion: The intervention given has equally effective statistically in Group-A and Group-B.
Keywords: Kolakulatthadi Churna Pinda Sweda , Ansasandhi Shula, Ansa Sthabdata, Bahu Shosha
Introduction
Avabahuka is a disease that usually affects the shoulder joint (Amsa Sandhi) and is produced by the Vata dosha. Loss of Bahu praspandana, stambha and shula at the shoulder joint are the cardinal feature of Avabahuka. Even though the term Avabahuka is not mentioned in Nanatmaja vata vyadhi, Acharya Sushruta have considered Avabahuka as a Vata Vyadhi. Apabahuka in modern can be correlated to Frozen Shoulder. In the realm of conventional medicine this illness is managed by analgesics, physiotherapy, oral corticosteroids, intra articular corticosteroid injections, capsular distention, manipulation under anesthesia and arthroscopic capsular release. In Madhava Nidana two conditions of the disease has been mentioned, Ansa shosha and Avabahuka Ansa Shosha can be considered as the preliminary stage of the disease where loss or dryness of shleshka kapha at Ansa sandhi occurs .In the next stage of Avabahuka, due to the loss of Shleshka kapha symptoms like shula during movement, restricted movements etc. are manifested. In our science Vata Vyadhis can be relieved by therapies like Abhayanga, Swedana, Sneha Pana, Nasya Karma, Vasti Karma and Shamana Oushadhi Prayoga etc. Chikitsa Sutra of Apabahuka includes Nasya, Uttarabhouktika Snehapaana, Nasaapana, Shamanaushadhi Prayoga etc. The drugs that can resolve the samprapti of Apabahuka are advocated.
In the realm of conventional medicine this illness is managed by analgesics, physiotherapy, oral corticosteroids, intra articular corticosteroid injections, capsular distention, manipulation under anesthesia and arthroscopic capsular release. Frozen Shoulder occurs approximately 3 % in general population. Occurrence is rare in children. But more seen in people of age group 40-60, common in females than males. Frozen shoulder is more frequent in diabetic patient. Generally, sufferers go for usage of Analgesic, Corticosteroid and Anti- Inflammatory drugs. This approach may give only timely cure but not permanent relief of pain and long-term usage of NSAID’S and steroids cause secondary complication.
This approach may give only a timely cure but not permanent relief of the pain and the long-term usage NSAID’s and steroids for relieving pain may in later course lead to secondary complications like kidney failures, liver disorders and gastritis. Considering all above points, patient with Avabahuka undergoing ayurvedic treatment like Snehana, Swedana are more effective than other treatment modality, thus above study under taken titles as ‘ Comparative Study to Evaluate the Efficacy of Kolakulatthadi Churna Pinda Sweda and Erandmoola Churna Pinda Sweda on Avabahuka with special reference to Frozen Shoulder.
Objectives:
- To evaluate the Efficacy of Kolakulatthadi Churna Pinda Sweda on Avabahuka.
- To Evaluate Efficacy of Erandmoola Churna Pinda Sweda on Avabahuka.
- To compare the efficacy Kolakulatthadi Churna Pinda Sweda and Erandmoola Churna Pinda Sweda on Avabahuka
MATERIALS AND METHODS:
Study Design : A Randomized Comparative Clinical Study.
Inclusion criteria:
Patients aged between 20 to 60 years of either sex and having classical signs and symptoms of Avabahuka.
Exclusion criteria:
Patients with history of Fracture of Shoulder or other Physical injuries to the shoulder joint and contraindicated to Swedana vidhi.
Sample Size: Total 40 patients fulfilling the diagnostic Criteria of both sexes were selected for the study. They were randomly assigned into 2 equal groups A & B where,
Group A- 20 Patients received Kolakulatthadi Churna Pinda Sweda for 30 minute for 14 days.
Group B - 20 Patients received Erandmoola Churna Pinda Sweda for 30 minute for 14 days.
Assessment criteria:
Assessment criteria:
- Subjective parameters:
1 )Amsa Sandhi Shoola ( Pain)
|
Amsa Sandhi Shoola |
GRADE |
|
No Pain |
0 |
|
Mild Pain particularly on moving the shoulder but able to continue routine work without difficulty |
1 |
|
Moderate pain felt on movement & interfere routine works |
2 |
|
Severe pain felt on movement & also at rest , disturbing sleep, unable to carry most of the routine work |
3 |
2) Amsa Sthabdata
|
Amsa Sthabdata (Stiffness) |
GRADE |
|
No Stiffness |
0 |
|
Mild Stiffness particularly during shoulder movement able to continue routine work without difficulty |
1 |
|
Moderate Stiffness felt on move & unable to continue work |
2 |
|
Severe Stiffness particularly during shoulder movement & also at rest interfere routine work |
3 |
3) Bahu Shosha
|
Bahu Shosha |
GRADE |
|
No Wasting |
0 |
|
Mild Wasting, can do work |
1 |
|
Wasting present, work with difficulty |
2 |
|
Wasting present, cannot move |
3 |
4) Sanchari Vedana
|
Sanchari Vedana |
GRADE |
|
No Sanchari Vedana |
0 |
|
Mild Sanchari Vedana particularly on moving the shoulder |
1 |
|
Moderate Sanchari Vedana felt on movement hamper routine works |
2 |
|
Severe pain felt on movement, also at rest, disturbing sleep, unable to carry most of the routine work |
3 |
- Objective parameters:
- Hyper Extension
|
Degree |
Grade |
|
Up to 500 |
0 |
|
Up to 300 |
1 |
|
Up to 100 |
2 |
|
Cannot Hyper Extension |
3 |
- Forward Flexion
|
Gradation |
Grade |
|
Up to 1800 |
0 |
|
Up to 1350 |
1 |
|
Up to 900 |
2 |
|
Up to 450 |
3 |
|
Cannot flex |
4 |
- External Rotation
|
Gradation |
Grade |
|
Up to 900 |
0 |
|
Up to 600 |
1 |
|
Up to 300 |
2 |
|
Cannot rotate |
3 |

Table No.1 Age Wise Distribution of Patient of Avabahuka
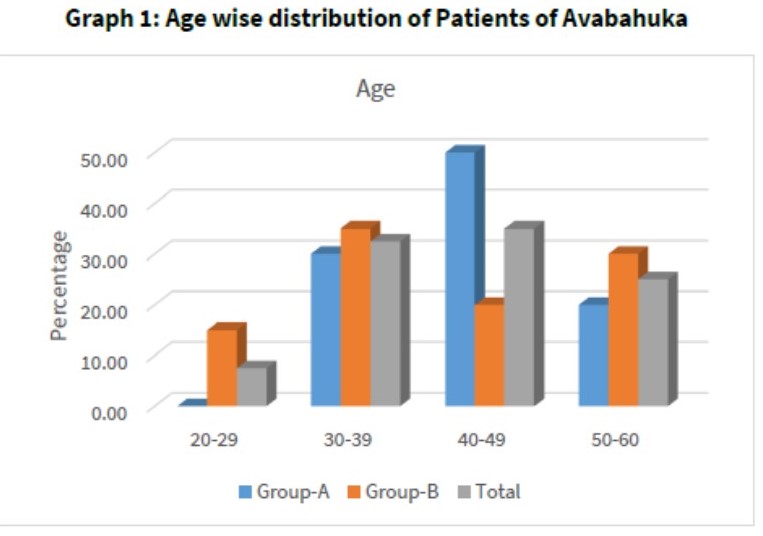
Graph 1: Age wise distribution of Patients of Avabahuka
Table No.2 Gender Wise Distribution of Patient of Avabahuka
Graph.2 Gender Wise Distribution of Patient of Avabahuka
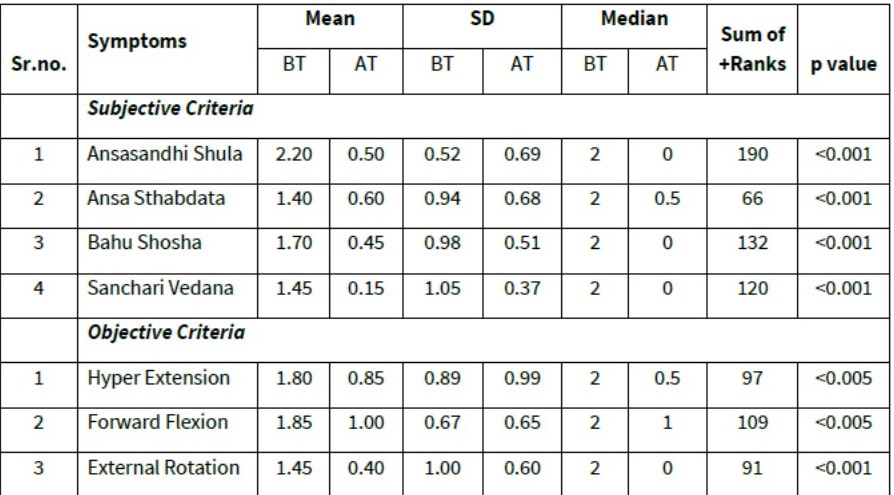
Table No.3 Wilcoxon Signed Rank Test Of Symptom score of Avabahuka of Group-A
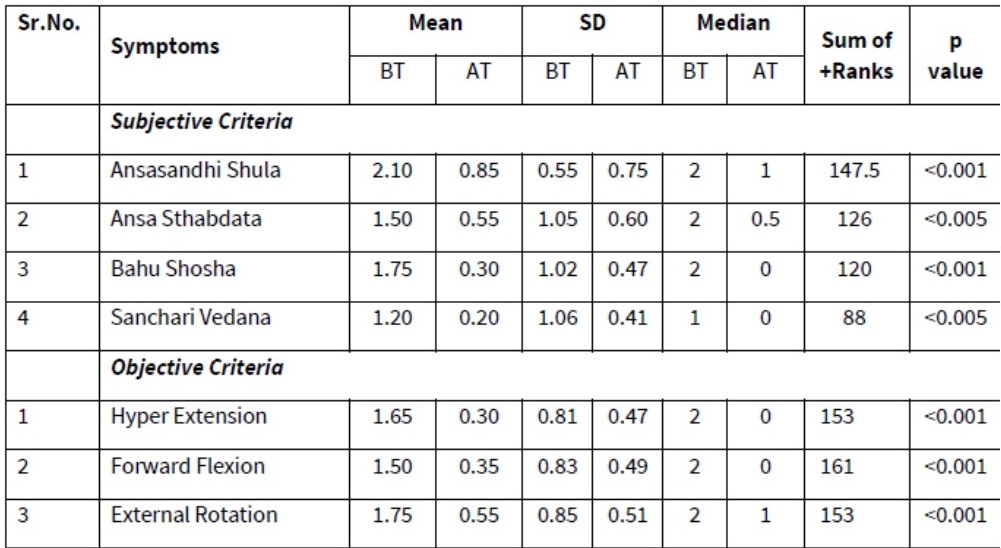
Table No.4 Wilcoxon Signed Rank Test of Symptom score of Avabahuka of Group-B :
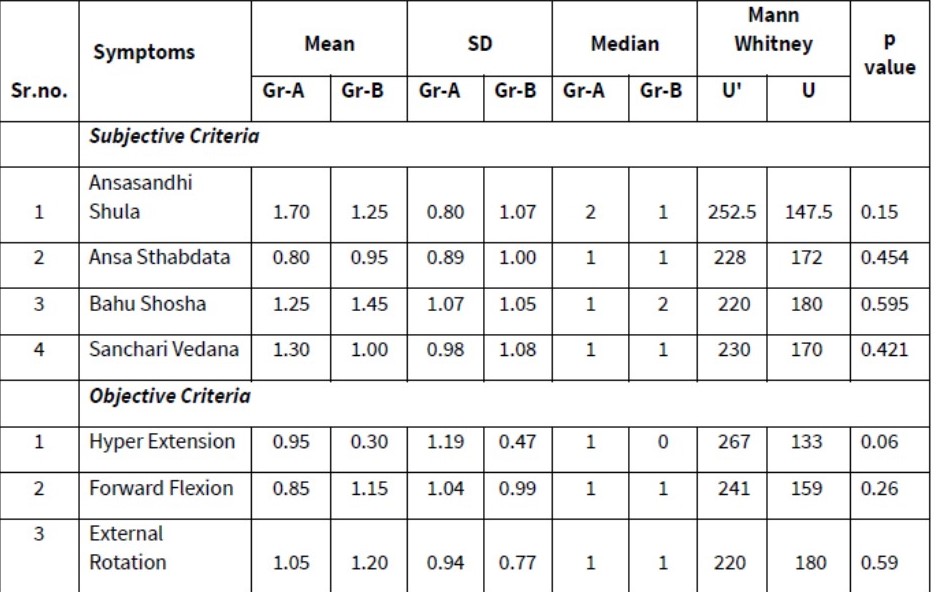
Table No.5 Comparison between Two Group w.r.t Symptoms Score of 40 Patients of Avabahuka By Mann-Whitney ‘U’ Test
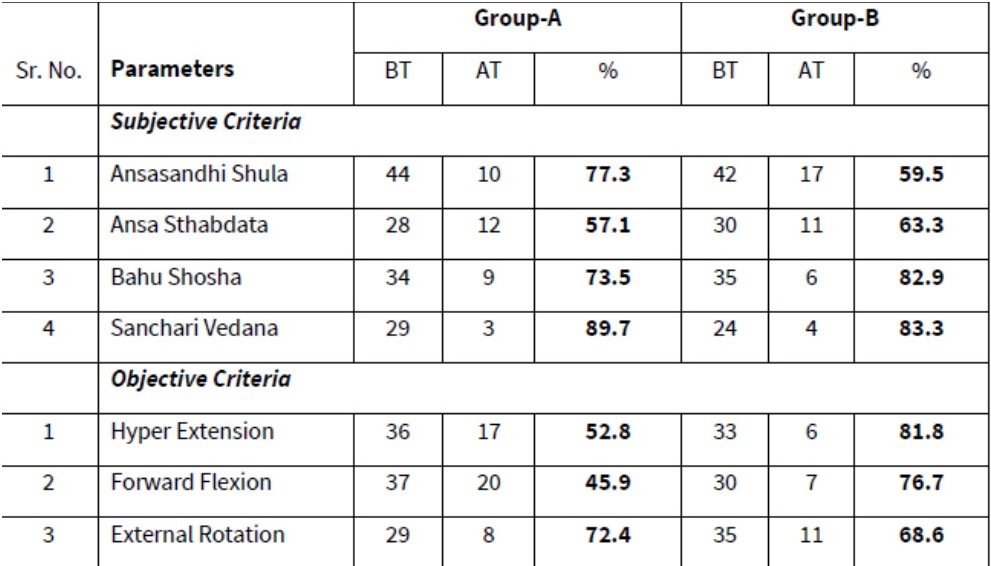
Table No.7 Percentage of Relief (Subjective Criteria) in Each Symptom of Avabahuka
As per inclusion criteria of patients were selected having age between 20 years to 40 yrs. and distributed it in four-sub age groups. Out of 40 patients, number of patients found in age group 20-29 were 03[7.5%], in 30 to 39 yrs. were 13 [32.5%], in age group 40-49 yrs. were 14[35%], in age group 50- 60 yrs. were 10 [25%], in numbers and percentage respectively.In this study , there were 21[52.5%] male while 19[47.5%] while female.
The Difference between before treatment and after treatment score of both groups compared by ‘Mann-Whitney U Test’. It was found that the sum of rank of Group-A for the symptom Ansasandhi Shula was 252.5, Test statistic (U) was 147, where the test statistic U was lies between Population Mean ± 1.96 SD which is not significant at 5% level of significance. (p >0.05) Therefore the difference between Symptom Score of Ansasandhi Shula of Group-A and Group-B is statistically not significant, so therefore we can conclude that in the symptom Ansasandhi Shula, so both groups were equally effective.
In symptoms Ansa Sthabdata, Bahu Shosha, Sanchari Vedana p value obtained is < 0.05 where test statistic U value it was between lies Population Mean ±1.96 SD which shows difference was considerably not significant, so therefore we can conclude that in these symptoms i.e. Ansasandhi Shula and, Bahu Shosha, both drug has found equally effective statistically.
However, it was found in the parameters like Hyper Extension, Forward Flexion, External Rotation Test statistic (U’) was not between Population Mean ±1.96 SD which is not significant at 5% level of significance. (p >0.05) Therefore the difference between Score for these parameters in Group-A and Group-B is statistically not significant, so therefore we can conclude that in these symptoms interventional drug has equally effective statistically in Group-A and Group-B.
Percentage of Relief in Symptoms Score: (Subjective Criteria)
In Group-A, percentage of relief noted in Ansasandhi Shula was 77.3%, while relief observed in Ansa Sthabdata, Bahu Shosha, Sanchari vedana, Hyper Extension, Forward Flexion, External Rotation, it was 57.1%, 73.5%, 89.7%, 52.8%, 45.9%,and 72.4 % respectively.
In Group-B, percentage of relief observed in Ansasandhi Shula was 59.5%, while relief observed in Ansa Sthabdata, Bahu Shosha, Hyper Extension, Forward Flexion, External Rotation it was 63.3,%, 82.9%, 83.3%, 81.8%, 76.7%and 68.6 % respectively.
Average relief observed in Group-A in subjective criteria was 74.4% while in objective criteria it was 57%. Average relief in both criteria was 67%.
Average relief observed in Group -B in subjective criteria was 72.3% while in objective criteria it was 75.7%. Average relief in both criteria was 73.7%.
Discussion
Age: As per inclusion criteria of patients were selected having age between 20 years to 40 yrs. and distributed it in four-sub age groups. Out of 40 patients, number of patients found in age group 20-29 were 03[7.5%], in 30 to 39 yrs. were 13 [32.5%], in age group 40-49 yrs. were 14[35%], in age group 50- 60 yrs. were 10 [25%], in numbers and percentage respectively.
Gender: In this study , there were 21[52.5%] male while 19[47.5%] while female.Incidence of male was observed more.
Religion : Out of 40 patients in the study maximum number of patients were found in Hindu religion, they were 29[72.5%], 02[5%] were from Muslim religion, 9[22.5%] were belong to Budhha religion it may due to population distribution. Religion has no any specific co relation with the incidence of the condition.
Education: Education Status shows that out of 40 patients, 05 [12.5%] were uneducated, 9[22.5%] up to primary education, 11[27.5%] were up to SSC, 11[27.5%] were up to HSC level while 04 [10%] patients were having education up to graduate level.
Occupation: Occupation status – In this study out of 40 patients 25 [62.5%] were indulging labor type of work, 7[17%] were having manual type of work while 8[20%] were Hving sedentary type of work. More were labour in this study.More patienst were involving in labour work, may be one the causative factor responsible for the Avbahuk.
Discussion Clinical Observations:
Effect of Therapy on Symptoms of Avabahuka in Group-A Statistically:-
The Wilcoxon signed-rank test is a non-parametric test for the case of two related samples or repeated measurements on a single sample. For the analysis of subjective criteria in Group-A the Wilcoxon Signed Rank Test was applied for Symptom score of Avabahuka, and findings are as follows.
- Subjective criteria:
In Group-A, regarding symptom Ansasandhi Shula, Ansa Sthabdata, Bahu Shosha, and Sanchari Vedana, p value observed was <0.001 which was statistically highly significant (p<0.001).
- Objective Criteria:
In symptom Hyper Extension, Forward Flexion, External Rotation, p value observed was <0.001 which was statistically highly significant (p<0.001). The Mean ± SD value obtained Before Treatment (BT) was and After Treatment (AT) it was changed and it was was statistically highly significant (p<0.001).
Effect of Therapy on Symptoms of Avabahuka in Group-B Statistically: -
- Subjective criteria:
In Group-B regarding symptom Ansasandhi Shula, Ansa Sthabdata, Bahu Shosha, and Sanchari Vedana, p value observed was <0.001 which was statistically highly significant (p<0.001).
- Objective Criteria:
In symptom Hyper Extension, Forward Flexion, External Rotation, p value observed was <0.001 which was statistically highly significant (p<0.001). The Mean ± SD value obtained Before Treatment (BT) was and After Treatment (AT) it was changed and it was statistically highly significant (p<0.001).
Comparison between Two Group in Symptoms Score:
It was found that the sum of rank of Group-A for the symptom Ansasandhi which is not significant at 5% level of significance. (p >0.05) Therefore the difference between Symptom Score of Ansasandhi Shula of Group-A and Group-B is statistically not significant, so therefore we can conclude that in the symptom Ansasandhi Shula, so both groups were equally effective.
In symptoms Ansa Sthabdata, Bahu Shosha, Sanchari Vedana p value obtained is < 0.05 which shows difference was considerably significant and the mean was more in group A for both the symptoms, so therefore we can conclude that in these both symptoms i.e. Ansasandhi Shula and, Bahu Shosha, trial drug has found effective compare to group -B statistically.
However, it was found in the parameters like Hyper Extension, Forward Flexion, External Rotation which is not significant at 5% level of significance. (p >0.05) Therefore the difference between Score for these parameters in Group-A and Group-B is statistically not significant, so therefore we can conclude that in these symptoms interventional drug has equally effective statistically in Group-A and Group-B.
Percentage of Relief in Symptoms Score:
Average relief observed in Group-A in subjective criteria was 74.4% while in objective criteria it was 57%. Average relief in both criteria was 67%. Average relief observed in Group -B in subjective criteria was 72.3% while in objective criteria it was 75.7%. Average relief in both criteria was 73.7%.
Mode of action of the Swedan:
In Avabahuka there is provocation of vata dosha. So, to deactivate vaatdosha we need to do vatnashaman upakrama. After doing Pindaswedan due to its properties and local effects it is useful in this disease. It is easy to use. Due to the presence Kolakulatthadi Churna and Erandmula churna pindasweda which is best vatanashak, it acts as a going through the arterial vasodilation. Arteriol vasodilation is the process of relaxation of smooth muscle in arteriolar wall allowing increased blood flow through the artery. This redirects the blood into the superficial capillaries in the skin increasing heat loss by convection and conduction. Body needs to maintain a mean temperature for internal organs therefore it attempts to set an equilibrium. Hence it relaxes the muscles and make it comfort from Pain and spasm.
Limitation and scope of study:
The sample size was small to draw a generalized conclusion. Therefore, the Pindasweda therapy along with other Panchakarma like Basti can be tried in a large sample for an appropriate duration and to prove efficacy of this intervention.
Conclusion
It was observed that, in Group-A and Group B, regarding symptom Ansasandhi Shula, Ansa Sthabdata, Bahu Shosha and Sancharivedana was statistically highly significant within group. In symptoms Ansasandhi Shula, Ansa Sthabdata, Bahu shosha, Sancharivedana shows difference was considerably not significant. So therefore, we can conclude that in these symptoms i.e., Ansasandhi Shula and, Bahu Shosha, both drugs have found equally effective statistically.
However, it was found in the parameters like Hyper Extension, Forward Flexion, External Rotation the Score for these parameters in Group-A and Group-B is statistically not significant, so therefore we can conclude that in these symptoms the intervention given has equally effective statistically in Group-A and Group-B.
References
value="
- Agnivesha, Charaka Samhita, Sutrasthana,Acharya Jadavji Trikamji, Choukambha publication, 2001 Varanasi. Pg no.78.
- Agnivesha, Charaka Samhita, ChikitsaSthana, chapt 28, Acharya Jadavji Trikamji, Choukambha publication, 2001 Varanasi. Pg no.616
- Sushruta, Sushruta Samhita, Chikitsasthanna, chapt 5, sloka no 23 Acharya Jadavji Trikamji, Choukambha Orientalia 2003 Varanasi. Pp824.
- Sushruta, Sushruta Samhita, Chikitsasthanna,chapt 5,sloka no 23 Acharya Jadavji Trikamji, Choukambha Orientalia 2003 Varanasi. Pp824.
- Vagbhatacharya, Ashtanga Hrudaya, Nidanasthana,chap 15,Pandit. Bhisagacharya Harishastri Paradkar vaidya, Nirnay Sagar Press, 2002, Varanasi, Pp-956.
- Maadhavakara, Maadhava Nidaanam, Vatavyadhinidana,chapt 22,sloka 64, Prof. K.R. Srikanta Moorthy, Chaukambha Orientalia, 1993, Varanasi, Page no.404
- Sharangadhara, Sharangadhara Samhita, VaidhyaSagar Pandit Parasurama sastri, Choukhambha Orientalia, 2002, Varanasi, Page no103
- Bhavamisra, Bhava Prakasha Nigantu, Dr. G.S.Pandey, Choukhambha Bharati Academy, 2004, Varanasi, Pp-984, Page No.226
- Arunadatta, Ashtanga Hrudaya, Pandit. Bhisagacharya Harishastri paradkar vaidya, Nirnay Sagar Press, 2002, Varanasi, Page no.534
- Govindadas, Bhaishajya Ratnavali, Chaukhamba samskrita samsthan, Varanasi, 2000, page no.373
- Sushruta, Sushruta Samhita, Acharya Jadavji Trikamji, Choukambha Orientalia 2003 Varanasi. Page no.269
"
