Original Article
Year: 2020 |Volume: 1 | Issue: 8 |Pages: 317-329
Apamarga Ksharasutra In Management of Fistula in- Ano : A Clinical Study
About Author
Correspondence Address:
Dr Apeksha P Moray, PG Scholar, Department of Shalya Tantra, Dr. V J D Gramin Ayurved Mahavidyalaya Patur, Email: apmoray21@gmail.com mobile no. 7588084403
Date of Acceptance: 2020-11-20
Date of Publication:2020-12-01
Article-ID:IJIM_41_12_20 http://ijim.co.in
Source of Support: NIL
Conflict of Interest: NIL
How To Cite This Article: Moray Apeskha & et.al. . Apamarga Ksharasutra In Management of Fistula in- Ano : A Clinical Study Int. J Ind. Med. 2020;1(8):317-329
Abstract
Background: The Bhagandara is one among the eight Mahagadas described by Acharya Sushruta. ‘Fistula-in-ano is an abnormal hollow tract or cavity that is lined with granulation tissue and that connects a primary opening inside the anal canal. Methods: Patients of either sex or age group between 20 to 60 years. Ksharsutra Treatment is given for the periods of 3 months. In addition, treatment was continued beyond 3 months if not healed but observations will be noted up to 3 months only. Observations and Results : Bhagandar is present mainly in age group 35 to 50 years, Pain during defecation is reduced in significantly in subsequent follow up of Ksharsutra. Ksharsutra treatment was effective in reducing discharge from wound site. Bleeding from wound site was effectively reduced, cutting rate was good and Fistula in ano tract was cut highly significantly. Conclusion: Ksharsutra application is effective in relieving Fistula in-ano.
Keywords: Ksharsutra, Bhagandara, Fistula in ano, Bleeding, Mahagadas
Introduction
‘Fistula-in-ano is a strange empty parcel or pit that is fixed with granulation tissue and that associates an essential opening inside the anal canal to a secondary opening in the perianal skin; secondary tracts may be many and can extend from the same primary opening. [1]. The Bhagandara is one among the eight Mahagadas described by Acharya Sushruta. In Vedic period no clear-cut description is found but the Samhitas and Puranas do have abundant evidences regarding the existence and treatment of this disease. The true prevalence of fistula in ano is unknown. One study showed that the prevalence of fistula in ano is 8.6 cases per 100,000 population. Treatment of fistula-in-ano remains challenging[2]. Surgery is the treatment of choice, with the goals of draining infection, eradicating the fistulous tract, and avoiding persistent or recurrent disease while preserving anal sphincter function[3],[4] but it has its own limitation with higher recurrence rate. Otherwise, application of chemical Seton named “Ksharasutra” (a medicated cotton thread coated with Ayurvedic medicines) is mentioned in the ancient samhitas[5]. Application and follow-up of Ksharasutra are very easy, require lesser hospital stay, lesser pain, have very low rate of difficulties and most importantly cost effective. Current study shows results of 30 cases of fistula in ano treated with Ksharasutra.
MATERIAL AND METHOD
Selection Of Patients :
All the patients of fistula in ano who attended O.P.D and I.P.D. of our College and Hospital and willing for Ayurvedic treatment only, were selected irrespective of sex, occupation duration of complaints etc.
Inclusion criteria :
1) Patients of either sex or age group between 20 to 60 years
2) Patient suffering from fistula in ano with presenting sign and symptoms. e.g. Bloody or foul-smelling drainage (pus) from an opening around the anus, Recurrent anal abscesses, Irritation of the skin around the anus, feve, Pain and swelling around anal region.
3) Patients ready to give informed written consent only selected.
Exclusion criteria :
1) Patients taking other treatment from any pathy for the same problem during clinical trial.
2) Pregnant and lactating females and children.
3) Serious systemic disease i.e. DM, TB, Syphilis, HIV, Hepatitis B.
4) Carcinoma of rectum, proctalgia fugax, chron’s disease, internal & external haemorrhoid, fissure & where it is contraindicated
Treatment of subject:
Period - 3 months (Ksharasutra every 7th day for 3 months)
Treatment of subject was stopped before 3 months if fistula is healed. In addition, treatment was continued beyond 3 months if not healed but observations will be noted up to 3 months only.
Procedure of placing Ksharasutra
A long metallic malleable probe with an eye is introduced through the external opening and attempted to pass the tip of probe through the internal opening. Care is taken not to open false track. The eye of the probe is threaded with Ksharasutra and probe is gently removed, so the entire tract is edge through medicated Ksharasutra. Following which the two ends of the thread will tightly tied using two knots outside the anal canal.
Changing of Ksharasutra
The thread is changed at weekly interval and slowly tightened. A new Ksharasutra is applied by rail-road technique[6].
Pathya
Hot sitz bath twice a day, Advice the patient to keep the local site hygienically clean.
Laxative – Dabur Avipattikar Churna[9] 2 - 6 gm at bed time with lukewarm water.
Dietary control was advice.
Criteria of assessing the improvement :
postoperative pain was evaluated by visual analog scale. The length of old thread was measured to know the length of cutting of fistulous tract. Gradually, the thread cuts out of the tract with a healed wound
Cutting rate of Ksharsutra = Length of Ksharsutra in first setting/ No. Of weeks for healing (cm/week)
Pain As per VAS Score[7]
|
Pain score |
Grade |
|
0 |
No pain |
|
1-3 |
Mild pain |
|
4-6 |
Moderate pain |
|
7-10 |
Severe pain |
Discharge [8] –
Severe : Changing sanitary pads or cotton pads minimum 2 times a day
Moderate : Changing of pads once a day only
Mild : No requirement of pads
Nil : Area is completely dry
Follow up: every 7th day.
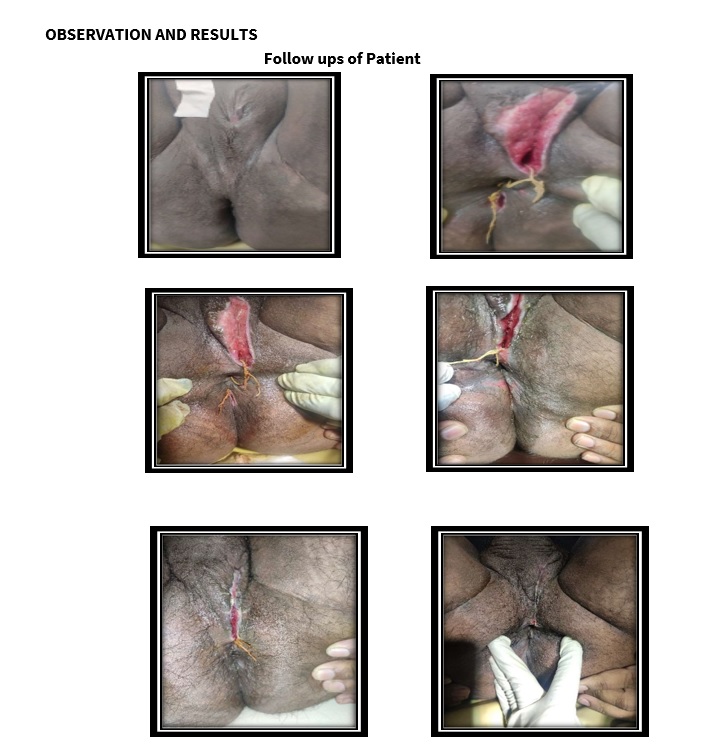
follow up
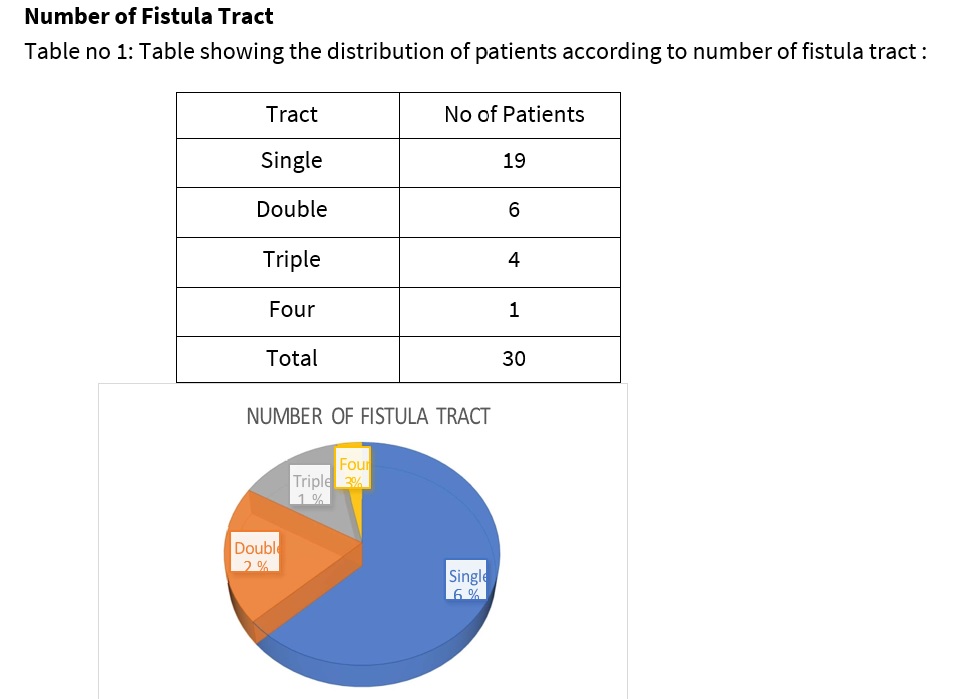
table 1
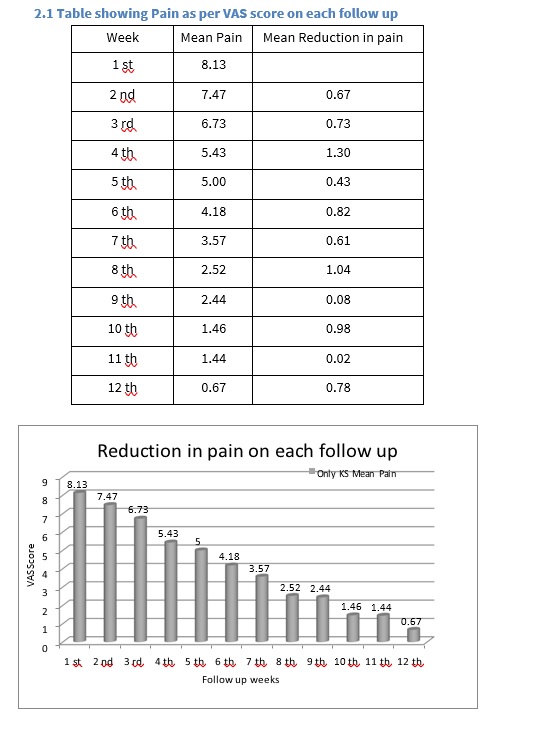
table 2
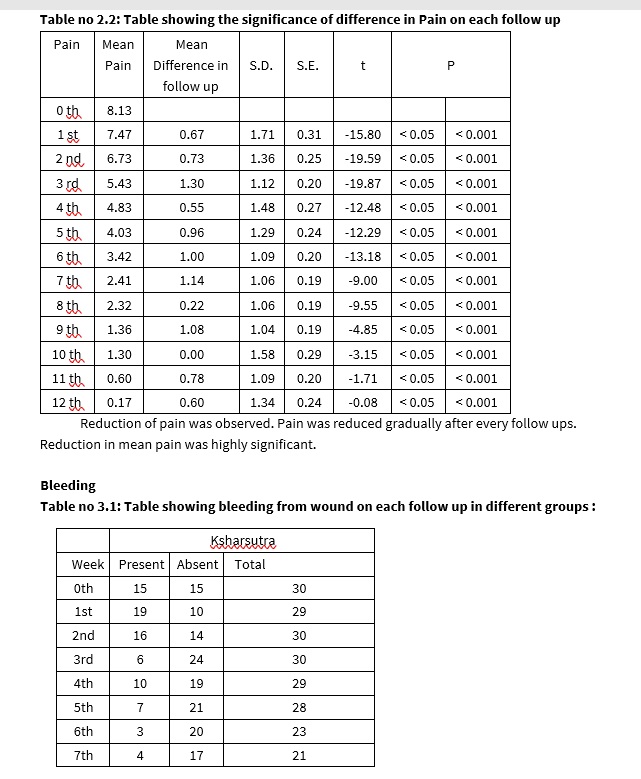
table 3
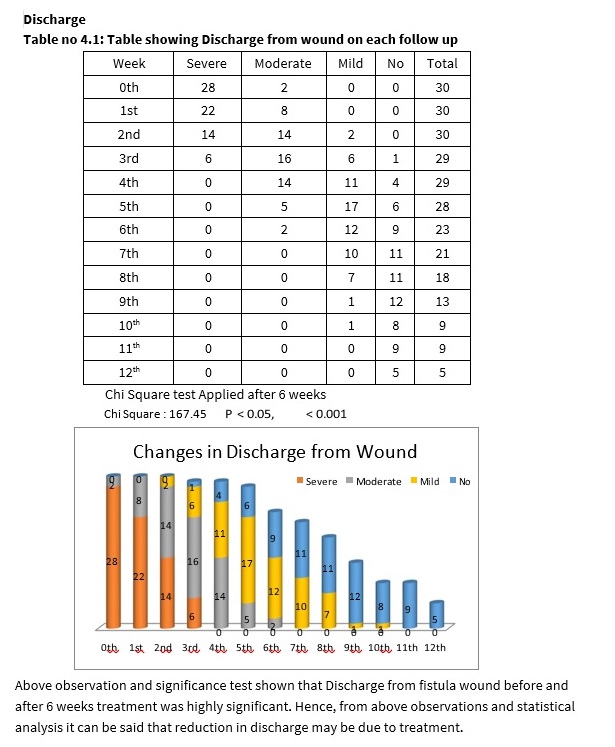
table 4
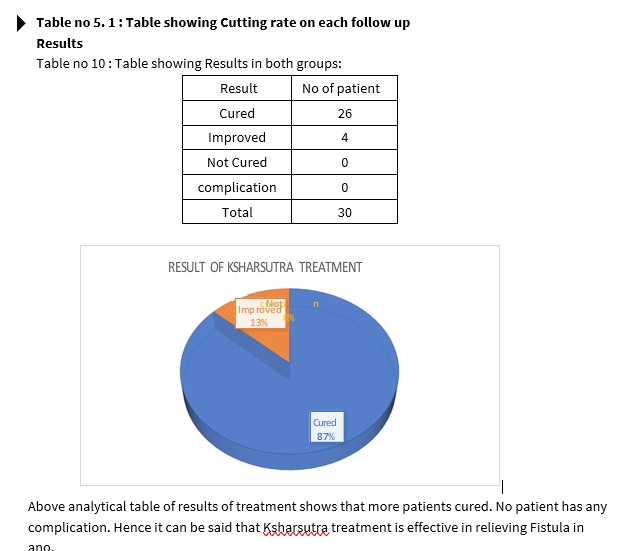
table 5
Discussion
1) Number of fistula in ano
Patients having single fistula in ano were more i.e. 19, while double were 6, Triple opening were 4 and more than 3 opening were in 1 patient. As chronicity increase number of opening may increase. This was observed that number of opening were increased in patient having more ignorance and chronicity towards disease.
In cited article number of external opening were single in 89 % cases and rest were more than single, in current study number of single tracts were about 60 %. In current study though patient with multiple opening are more but distributed equally in both groups.
2) Pain during defecation
Patients having maximum pain as per mean VAS score were on 0th day. Pain was decreased on each follow up. Significance test shown that difference of mean VAS score before and after treatment was highly significant. Hence, it can be said that change occurred may be due to treatment.
Also, as treatment course advances patient’s threshold towards pain also increases hence patient feels like reduction in pain. Also, Sitz bath after defecation also increases relief due to reducing inflammation.
3) Bleeding from wound site
Reduction of bleeding after treatment was highly significant. Hence, it can be said that change occurred may be due to treatment.
4) Discharge from Wound :
It was observed that Discharge from fistula wound before and after 6 weeks treatment was reduced highly significantly. Hence, from above observations and statistical analysis it can be said that reduction in discharge may be due to treatment.
5) Cutting Rate
Above observation and significance test shown that cutting rate was highly significant. Fistula tract was reducing on every follow up. Cutting rate was equivocal with previous study. Cutting rate was nearly 0.61 cm/ week.
Probable mode of action of drug:
Ayurveda View
Pain -Sitz bath with warm water : It worked in relieving vitiation of Vata and relieving spasm and localised inflammation at wound site. This also helps in reducing contamination at site of wound.
Pathya and Avipattikar Churna were useful for relieving Agnimandya and helped smooth passage of stool. This ultimately helped in healing of wound at anal region and relieving pain during defecation.
Discharge- Reduction in discharge was secondary with increase in healing of wound due to Ksharasutra discharge was simultaneously reducing. Hence effect of decrease in discharge was observed.
Bleeding from wound site:
This may be due to Vranaropak, Vranashodhak, Shothahar effect of drugs and Ksharasutra. Also as follow up underwent with Ksharasutra healing was also associated which helped in reduction of discharge from wound site.
Cutting Rate -Ksharasutra is well known for its cutting rate. Standard cutting rate of Ksharasutra was noted as 0.5 cm/week, but in current study it was observed at nearly 0.61 cm/week. This may be due to difference in technique of tightening of Ksharasutra. Also, slight difference may be due to concentration of Ksharasutra and its storage technique. This property should be studied as a further scope of study. Both groups had nearly equal cutting rate. So, this may be said that dhoopan does not interfere with cutting rate of Ksharasutra.
Conclusion
1. Bhagandar is present mainly in age group 35 to 50 years, with sex wise more incidence in male and having more non-vegetarian diet.
2) Pain during defecation is reduced in significantly in subsequent follow up of Ksharasutra.
3) Ksharasutra treatment was effective in reducing discharge from wound site.
4) Bleeding from wound site was effectively reduced on subsequent follow ups.
5) Cutting rate was good and Fistula in ano tract was cut highly significantly. Hence it can be said that treatment is effective in relieving Fistula in ano
References
value="
1. Author: Juan L Poggio, MD, MS, FACS, FASCRS; Chief Editor: John Geibel, MD, DSc, MSc, AGAF Fistula-in-Ano https://emedicine.medscape.com/article/ 190234overvie
2. Phillips J, Lees N, Arnall F. Current management of fistula-in-ano. Br J Hosp Med (Lond). 2015 Mar. 76 (3):142, 144-7. [Medline] Sainio P. Fistula in ano in a defined population. Incidence and epidemiological aspects. Ann Chir Gynaecol, 1984. 73(4) 219-24
3. Vasilevsky CA, Gordon PH. Benign Anorectal: Abscess and Fistula. Wolff BG, Fleshman JW, Beck DE, Pemberton JH, Wexner SD, eds. The ASCRS Textbook of Colon and Rectal Surgery. New York, NY: Springer; 2007. Chapter 13.
4. Williams JG, Farrands PA, Williams AB, et al. The treatment of anal fistula: ACPGBI position statement. Colorectal Dis. 2007 Oct. 9 Suppl 4:18-50. [Medline]
5. Multicentric randomized controlled clinical trial of Kshaarasootra (Ayurvedic medicated thread) in the management of fistula-in-ano. Indian Council of Medical Research. Indian J Med Res. 1991 Jun; 94():177-85.[PubMed] [Ref list
6. Dutta G, Bain J, Ray AK, Dey S, Das N, Das B. Comparing Ksharasutra (Ayurvedic Seton) and open fistulotomy in the management of fistula-in-ano. Journal of Natural Science, Biology, and Medicine. 2015;6(2):406-410. doi:10.4103/0976-9668.160022.
7. Shastri L, Yogratnakara, VidyotiniTika,Uttarardh; Yonivyapadachikitsa 5. Varanasi: Chaukhamba Prakashana, Reprint Edition 2013: 409. ],[ Sahara Shrestha: Dhoopana Karma: A Review Through Brihatrayi, International Ayurvedic Medical Journal (ISSN: 2320 5091) (February- March, 2017) 1(3)]
8. Evolution of antimicrobial and antifungal property of dhoopana karma (fumigation)
– by “dhup”an ayurvedic dhoopana product” by L. Sumitha and B. S Prasad,
Department of Bhaishajya Kalpana, Dept of Panchakarma, KLEU SBMK Ayurveda Mahavidhyalaya, Shahapur, Belgaum, Karnataka, India. IJPSR, 2015; Vol. 6(7): 2950 – 2954
9. Dabur Avipattikar Churna
10. “Comparative clinical study in the management of Bhagandara (Fistula-In-Ano) with vasa kshara sutra and Apamarga ksharasutra” Desertation for M.S.(Ayurveda) Shalyatantra Samanya, Rajiv Gandhi University of Health Science Nashik. By Vd.
Kshirsagar Nagendra 2011
11. Author: Juan L Poggio, MD, MS, FACS, FASCRS; Chief Editor: John Geibel, MD, DSc,
MSc, AGAF Fistula-in-Ano https://emedicine.medscape.com/article/190234-overvie
12. Phillips J, Lees N, Arnall F. Current management of fistula-in-ano. Br J Hosp Med (Lond). 2015 Mar. 76 (3):142, 144-7. [Medline]
13. Sainio P. Fistula in ano in a defined population. Incidence and epidemiological aspects. Ann Chir Gynaecol, 1984. 73(4) 219-24.
14. Vasilevsky CA, Gordon PH. Benign Anorectal: Abscess and Fistula. Wolff BG, Fleshman JW, Beck DE, Pemberton JH, Wexner SD, eds. The ASCRS Textbook of Colon and Rectal Surgery. New York, NY: Springer; 2007. Chapter 13.
15. Williams JG, Farrands PA, Williams AB, et al. The treatment of anal fistula: ACPGBI position statement. Colorectal Dis. 2007 Oct. 9 Suppl 4:18-50. [Medline]
"
